FRONTIERS IN MEDICAL CASE REPORTS - Volume 6; Issue 2, (Mar-Apr, 2025)
Pages: 01-09
Print Article
Download XML Download PDF
A Case of Incidentally Diagnosed Squamous Cell Carcinoma Arising from Mature Cystic Teratoma of Ovary in A Resource Limited Setup: Case Report and Literature Review
Author: Birhanu Kassie Reta, Nebiat Zerabiruk Embaye, Musie Negasi Gebreslase, Tsegay Gebremichael Gebremariam, Abrham Hagos Dimtsu, Yordanos Birhane Gebrecherkos
Category: Medical Case Reports
Abstract:
Malignant transformation is rare in mature cystic teratoma of the ovary (MCTO) with an incidence of 0.17-2%. The aim of this case report is to highlight the significance of considering malignant transformation of mature cystic teratoma in postmenopausal women. We present a case of a 65-year-old postmenopausal woman who presented with a complaint of a painful right lower abdominal swelling of 2 years duration with a recent increment in size. On an ultrasound scan there was a right adnexal complex cystic mass with focal cyst wall thickening and diffuse increased echogenicity. Total abdominal hysterectomy with bilateral salpingo-oophorectomy and omentectomy was done, and subsequent histopathologic examination confirmed squamous cell carcinoma arising from MCTO. A final diagnosis of FIGO stage IA squamous cell carcinoma was made; she took adjuvant chemotherapy, and she is currently in good health. In a clinically suspected case of ovarian mature cystic teratoma in a postmenopausal woman presenting with a painful adnexal mass with a recent increment in size and sonographic finding of cyst wall thickening, malignant transformation should be considered preoperatively to ensure proper surgical management and adjuvant chemotherapy. The aim of this study is to highlight the predictors of malignant transformation in mature cystic teratoma of the ovary and underscore the significance of referring patients to better setups for appropriate workup and management.
Keywords: Squamous Cell Carcinoma, Ovary, Mature Cystic Teratoma, Malignant, Transformation
DOI URL: https://dx.doi.org/10.47746/FMCR.2025.6201
Full Text:
Introduction
The ovarian tumor known as mature cystic teratoma of the ovary (MCTO) is composed of germ cell layers that have undergone full differentiation. Sixty percent of all benign ovarian tumors are this tumor, commonly referred to as dermoid cyst (Ahmed and Lotfollahzadeh, 2025; Atabekoglu et al., 2005). There is still much to learn about the pathophysiology and aetiology of MCTO. While some patients have no symptoms, others typically show up with constipation, a visible abdominal or pelvic mass, and abdominal pain and distension (Avci et al., 2012). Malignant transformation from MCTO is uncommon; just 1.4% of instances have been documented (Avci et al., 2012).
Malignant transformation in MCTO commonly occurs between the ages of 40 and 55, which is 10 years older than women with benign ovarian tumors, according to case reports (Sibarani et al., 2023). In the literature, squamous cell carcinoma (SCC) is the most common documented malignant transformation in MCTO (Goudeli et al., 2017; Tehranian et al., 2021). It is frequent for postmenopausal women to have SCC developing in MCTO (Tehranian et al., 2021; Dorji et al., 2022). Squamous cell carcinoma accounts for 80% of malignancies arising from MCTO, whereas adenocarcinoma and melanoma are other common histologic types developing in MCTO (Qian et al., 2023; Huang et al., 2023). Several risk factors for malignant transformation have been proposed, including tumor size, patient age, image results, and increased blood markers (Goudeli et al., 2017).
Hereby we reported a 65 years old Ethiopian woman diagnosed with squamous cell carcinoma arising from MCTO postoperatively on histopathologic examination. Due to the fact that there are increasing reports of malignant transformation of MCTO in postmenopausal women, clinicians should consider the possibility of malignancy preoperatively in a possible case of MCTO, especially in poorly established setups like ours, where serum biomarkers, CT scan, or MRI are not available. The aim of this study is to highlight the predictors of malignant transformation in mature cystic teratoma of the ovary and underscore the significance of referring patients to better setups for appropriate workup and management.
Case Presentation
History and Physical examination
A 65-year-old para 7 postmenopausal woman who is amenorrhoeic for the past 18 years presented to Aksum University Comprehensive Specialised Hospital with a complaint of right lower abdominal swelling of 2 years duration; associated with the swelling, she had a history of dull aching-type pain of the same duration. She claimed that the swelling has increased in size in the past 06 months. Otherwise, she has no history of vaginal bleeding, bowel or urinary complaints, weight or appetite loss, or swelling in other body parts. She has no family history of cancer. She has no significant past medical or surgical history. She denied a history of alcohol intake or cigarette smoking.
On physical examination, her vital signs were within normal range. Abdominopelvic examination revealed a soft mobile non tender well-delineated mass with a smooth surface at the right lower quadrant of the abdomen measuring, 17 cm x 12 cm.
Diagnostic Work Up
Abdominopelvic ultrasound scan demonstrated a right adnexal unilocular cystic mass with focal cyst wall thickening and diffuse increased echogenicity measuring 18.3 cm x 12 cm x 7.4 cm. Otherwise, the uterus, fallopian tubes, and contralateral ovaries are normal in size and shape. No other lesions are identified in the pelvic and abdominal cavity.
Computed tomography (CT) scan, magnetic resonance imaging (MRI), and serum markers (CA125, CA19-9, and CEA) were planned as a diagnostic workup for detection of possible malignancy, but all these investigation modalities were not available in our setup due to the low resources and war-induced economic crisis in our region.
With clinical diagnosis of benign right ovarian tumor like mature cystic teratoma, total abdominal hysterectomy (TAH) with bilateral salpingeo-ophrectomy (BSO) and omentectomy was done. The surgical specimens are subjected to histopathologic examination. Peritoneal wash cytology was also done, and the cytopathology report concluded negative for malignancy.
The pathologic examination grossly revealed grey brown cystic globular tissue with a smooth outer surface measuring 17 cm x 11 cm x 6.5 cm. The cut surface showed a unilocular cyst filled with sebum and keratinous content, with a focal area of solid focus measuring 4 cm x 3.9 cm x 2.2 cm (Fig. 1). Histologic sections through the cystic tissue displayed stratified squamous epithelium lined cyst with underlying cyst wall containing adipose tissue with solid sheets, nests, and cords of mild to moderately pleomorphic squamous cells with keratin pearl formation and scattered mitotic figures. Histologic sections through bilateral fallopian tubes, uterus, ovary, and omentum are unremarkable with no malignancy seen. With those findings, the histopathologic examination concluded squamous cell carcinoma arising from mature cystic teratoma. (Fig. 2 and Fig. 3)

Figure 1: Gross pathologic photographic image. A. showing unilocular cyst filled with sebum and keratinous material (arrow) and focal solid mass (star). B. Demonstrates the cut surface of the solid mass (arrow).
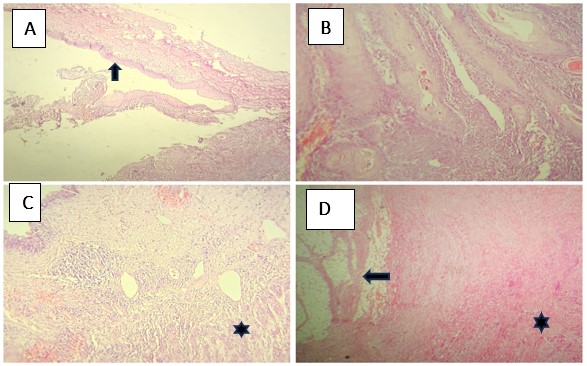
Figure 2: Microscopic images of hematoxylin and eosin (H and E) stained sections. A. 4x magnification displaying cyst wall lined by bland maturing squamous epithelium (arrow). B. 20x magnification displaying the squamous epithelial lining with keratinization. C. 4x magnification displaying stratified squamous epithelial lining with underlying proliferation of malignant squamous cells in cords and nests (Star). C. 4x magnification displaying the adipose tissue component of the mature teratoma (arrow) constituting the cyst wall being infiltrated by the malignant squamous cells (star).

Figure 3: Microscopic images of H and E sections. A. 20x magnification displaying nests and cords of mild to moderately pleomorphic squamous cells displaying intracellular and extracellular keratin pearl formation (arrow). (B and C). 20x magnification shows nests, cords, and trabecules of malignant squamous cells. D. 40x magnification displaying malignant squamous cords and trabecules with mitotic figures (arrow).
Therapeutic Intervention and Follow-Up
Based on the histopathology report, FIGO stage IA squamous cell carcinoma of the ovary is diagnosed; the patient is referred to Mekelle University Ayder Comprehensive Specialised Hospital for better investigation and management. Two months after the initial surgery, an abdominopelvic ultrasound and CT scan were done and confirmed no residual tumor. No distant metastasis or enlarged abdominopelvic lymph nodes are identified. The patient is counselled about the diagnosis, the stage of disease and prognosis, and the treatment modalities. Considering the postoperative diagnosis of the squamous cell carcinoma, the multidisciplinary team decided to give her chemotherapy, and she took six cycles of the paclitaxel and carboplatin regimen without significant complication. She is on follow-up every three months. Currently, at the time of writing the case report, she is in her first postoperative year, she is symptom free and actively participating in her social activities. The ultrasound and CT scan findings are normal.
Discussion
A benign tumor, MCTO, also referred to as a dermoid cyst, is the most prevalent germ cell ovarian neoplasm (Abhilasha et al., 2016). Women of childbearing age account for the majority of occurrences, while it can happen at any age. SCC accounts for the majority of instances, with MCTO malignant transformation occurring in only 2% of cases (Dorji et al., 2022). Adenocarcinoma and melanoma are among the additional histological variations (Qian et al., 2023; Huang et al., 2023).
A higher rate of cell proliferation leads to the development of cancerous cells, which leads to the malignant transformation of the tissue components in MCTO (Goudeli et al., 2017). It is unclear what specifically caused this malignant change (Li et al., 2019). According to case reports, women with benign MCTO are typically 10 years younger than those with malignant MCTO, with the former often being common between 40 and 55 years old (Sibarani et al., 2023). According to earlier studies, the average age of malignant change in MCTO was 53.5 years (Li et al., 2019), while there have been a few documented occurrences of SCC in women as young as 19 (Li et al., 2019).
In less than 1% of MCTO cases, squamous transformation is observed, especially in a postmenopausal woman with unilateral tumors. Women over 45 are said to have a worse prognosis than patients who are younger (Li et al., 2019). Most of the time, patients start out without any symptoms. Weight loss, changed bowel habit, urinary frequency, and abdominal pain and/or mass are some significant signs (Avci et al., 2012). Our patient is a 65-year-old postmenopausal woman, and the diagnosis of squamous cell carcinoma is made postoperatively, but we should have suspected malignancy preoperatively, and the patient should have been referred to a better setup for optimal preoperative investigation.
Regretfully, there are no particular image results, serum markers, or clinical indications to identify malignant transition in MCTO prior to surgery (Toba et al., 2020). Age, postmenopausal status, increased tumor size and invasion, elevated levels of certain tumor markers (CA 19-9, CEA, and CA 125), and tumor remnants are some proposed, albeit nonspecific, risk factors for this condition (Avci et al., 2012; Sibarani et al., 2023). However, histopathologic examination is the only way to confirm malignant transformation.
While TAH, BSO, and complete staging surgery are appropriate treatments, managing SCC malignant transformation of MCTO is difficult (Li et al., 2019; Zaboli et al., 2022). Women who were treated with chemotherapy and radiotherapy rather than surgery perished within the first year (Kashimura et al., 1989). A second operation should therefore be considered for individuals who were not staged optimally at the time of surgery, since thorough excision enhances the prognosis (Ahmed and Lotfollahzadeh, 2025). According to the evidence now available, TAH can considerably reduce the risk of death in SCC malignant transformation. Oddly enough, omentectomy also improved survival (Ramirez et al., 2021; Kalyani, 2022).
Early detection of the disease, particularly if it only affects the ovaries, is associated with a favorable prognosis and an overall survival rate of 100% and 75% (at 2 and 5 years, respectively) (Tseng et al., 1996; Shaffi et al., 2022; Chen et al., 2008).
Given the abundance of case reports in the literature about MCTO turning into malignancy, it should be evaluated as a possible differential diagnosis in older patients who have palpable adnexal mass and abdominal pain, as well as those with a large tumor diameter and cyst wall thickening on ultrasound examination.
Conclusion
In a clinically suspected case of ovarian mature cystic teratoma in a postmenopausal woman presenting with a painful adnexal mass with recent increment in size and sonographic finding of cyst wall thickening, malignant transformation should be considered preoperatively to ensure proper surgical management and adjuvant chemotherapy.
Abbreviations
MCTO: mature cystic teratoma of ovary
SCC: squamous cell carcinoma
CEA; carcinoembryonic antigen
CA-125; cancer antigen 125
CA 19-9: carbohydrate antigen 19-9
H and E: Hematoxylin and eosin
Acknowledgment: None
Authors’ Contribution: Birhanu Kassie Reta: Conceptualization, Visualization, Supervision, Writing- Original draft preparation. Nebiat Zerabiruk Embaye: Data curation, Writing- Original draft preparation. Musie Negasi Gebreslase: Visualization, Investigation. Tsegay Gebremichael Gebremariam: Investigation, Supervision. Abrham Hagos Dimtsu: Investigation, Validation. Yordanos Birhane Gebrecherkos: Investigation, supervision.
Funding: This study did not receive any grants or funding from either for-profit or non-profit organisation.
Data Availability Statement: The data is available from the corresponding author upon a reasonable request.
Conflict of Interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed Consent: Written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review by the editor-in-chief of this journal on request.
References:
Abhilasha N, Bafna U, Pallavi V, Rathod P, Krishnappa S. A review of squamous cell carcinoma arising in mature cystic teratoma of the ovary. Indian J Cancer 2016; 53: 612-614.
Ahmed A, Lotfollahzadeh S. Cystic teratoma. Treasure Island (FL): StatPearls Publishing; 2025.
Atabekoglu C, Bozaci E, Tezcan S. Elevated carbohydrate antigen 19-9 in a dermoid cyst. Int J Gynaecol Obstet 2005; 91: 262-263.
Avci S, Selcukbiricik F, Bilici A, Özkan G, Özagari AA, Borlu F. Squamous cell carcinoma arising in a mature cystic teratoma. Case Rep Obstet Gynecol 2012; 29: 282-284.
Chen RJ, Chen KY, Chang TC, Sheu BC, Chow SN, Huang SC. Prognosis and treatment of squamous cell carcinoma from a mature cystic teratoma of the ovary. J Formos Med Assoc 2008; 107: 857-868.
Dorji N, Choden S, Tshering S. Incidental diagnosis of squamous cell carcinoma transformation in mature cystic teratoma of the ovary: a case report and review of literature. SAGE Open Med Case Rep 2022; 10:2050313X221082426.
Goudeli C, Varytimiadi A, Koufopoulos N, Syrios J, Terzakis E. An ovarian mature cystic teratoma evolving in squamous cell carcinoma: a case report and review of the literature. Gynecol Oncol Rep 2017; 19: 27-30.
Huang X, Liao X, Chen X, Zeng Z. Squamous cell carcinoma, serous adenocarcinoma and osteosarcoma arising in a mature cystic teratoma of the ovary: a case report and literature review. 2023.
Kalyani P. Squamous-cell carcinoma in mature cystic teratoma of the ovary-a case report. Sch J Med Case Rep 2022; 9: 988-991.
Kashimura M, Shinohara M, Hirakawa T, Kamura T, Matsukuma K. Clinicopathologic study of squamous cell carcinoma of the ovary. Gynecol Oncol 1989; 34: 75-79.
Li C, Zhang Q, Zhang S, Dong R, Sun C, Qiu C, et al. Squamous cell carcinoma transformation in mature cystic teratoma of the ovary: a systematic review. BMC Cancer 2019; 19: 1-12.
Qian XQ, Chen LL, Zhu CK, Chen YX, Wan XY. Case report: squamous cell carcinoma and spindle cell sarcoma (SCS) arising in a mature cystic teratoma of the ovary. Front Surg 2023; 10: 1193994.
Ramirez AR, Arencibia-Sánchez O, Sánchez MA, Martinez AM, Laseca-Modrego M. Squamous cell carcinoma arising from a mature cystic teratoma of the ovary: a case report. Cureus 2021; 13: e12846.
Shaffi A, Keitany K, Itsura P, Odongo B, Kagendo N, Mburu A. Squamous cell carcinoma of the ovary arising in a mature cystic teratoma in a 28-year-old female: a case report and review of literature. South Afr J Gynaecol Oncol 2022; 14: 37-39.
Sibarani CNR, Permata HD, Martiana EF, Tjandraprawira KD, Hadinata CV. A rare case of squamous cell carcinoma transformation in a mature cystic teratoma of the ovary. SAGE Open Med Case Rep 2023; 11:2050313X231193305.
Tehranian A, Ghahghaei-Nezamabadi A, Seifollahi A, Kasraei S, Dehghani-Nejad H, Maleki-Hajiagha A. Ovarian mature cystic teratoma with malignant transformation: two case reports. J Med Case Rep 2021; 15: 1-6.
Toba N, Takahashi T, Ota K, Takanashi A, Iizawa Y, Endo Y, et al. Malignant transformation arising from mature cystic teratoma of the ovary presenting as ovarian torsion: a case report and literature review. Fukushima J Med Sci 2020; 66: 44-52.
Tseng CJ, Chou HH, Huang KG, Chang TC, Liang CC, Lai CH, Soong YK, Hsueh S, Pao CC. Squamous cell carcinoma arising in mature cystic teratoma of the ovary. Gynecol Oncol 1996; 63: 364-370.
Zaboli E, Heydari S, Alizadeh-Navaei R. Ovarian squamous cell carcinoma arising from mature cystic teratoma: a case report. Case Rep Clin Pract 2022; 7: 195-198.
|
